Impact Factor ISSN: 1837-9664

 Global reach, higher impact
Global reach, higher impactJ Cancer 2026; 17(6):1179-1186. doi:10.7150/jca.125480 This issue Cite
Review
Development of nasopharyngeal carcinoma target delineation: from two-dimensional radiotherapy to adaptive precision radiotherapy
Xiaojing Yang1,3, Lijun Liu1, Huicai Zhang1, Hanru Ren2 ![]() , Jie Fu1
, Jie Fu1 ![]()
1. Department of Radiation Oncology, Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China
2. Department of Orthopedics, Shanghai Pudong Hospital, Pudong Medical Center, Fudan University, Shanghai, China.
3. Division of Urology, Department of Surgery, Brigham and Women's Hospital & Harvard Medical School, Boston, MA, USA.
Received 2025-9-19; Accepted 2025-12-12; Published 2026-6-4
Abstract

Nasopharyngeal carcinoma (NPC) is mainly treated with radiotherapy. With the advancements of imaging and radiotherapy techniques, the delineation of NPC target areas has evolved from empirical field setting in the two-dimensional era to three-dimensional conformal radiotherapy (3D-CRT), intensity modulated radiotherapy (IMRT), and image-guided adaptive radiotherapy (ART), significantly improving treatment accuracy and safety. This review systematically explores the development process of target area delineation in NPC, focusing on the evolution and standardization of target areas in the nasopharynx and neck lymph nodes, and combines the role of multimodal imaging such as MRI and PET-CT in target area delineation. The article further examines the clinical response strategies and research trends of target area changes after induction chemotherapy (IC), and looks forward to the potential of ART and artificial intelligence in future target area delineation. The review aims to provide clinical practitioners with a scientific, rational, and personalized approach to target delineation, optimizing treatment plans and improving clinical outcomes.
Keywords: Nasopharyngeal carcinoma, Radiotherapy, Target delineation
Introduction
Nasopharyngeal carcinoma (NPC) is an epithelial derived malignant tumor originating from the nasopharyngeal mucosa, exhibiting distinct epidemiological, pathological, and biological characteristics [1]. Its incidence rate has obvious geographical distribution characteristics, which is relatively high in southern China (especially Guangdong and Guangxi), Southeast Asia, the Middle East and North Africa, and is closely related to EB virus infection, genetic factors and environmental exposure [2, 3].
Radiotherapy is the most important and effective curative treatment for NPC, especially for patients in stages I-III, offering favorable local control and long-term survival outcomes [4, 5]. The success of modern radiotherapy depends not only on the optimization of technical equipment and treatment plans, but also on the accurate delineation of the target area. Reasonable target delineation can minimize normal tissue damage while ensuring tumor control, thereby reducing complications and improving patients' quality of life (QoL) [6].
With the continuous advancement of imaging technologies such as CT, MRI, and PET-CT, radiotherapy technology has also developed from two-dimensional radiotherapy (2D-RT) to three-dimensional conformal radiotherapy (3D-CRT), intensity modulated radiotherapy (IMRT), image-guided radiotherapy (IGRT), and adaptive radiotherapy (ART) [7-9]. The target area delineation is gradually transitioning from "empiricism" to "evidence driven". Especially in recent years, with the widespread application of induction chemotherapy, tumor volume and morphology have undergone significant changes [10, 11], posing new challenges and adjustment strategies for target delineation.
This article intends to start with the target delineation during 2D-RT, summarize the technological evolution of NPC delineation, and focus on exploring the target delineation standards for nasopharyngeal and cervical lymphatic drainage areas in modern radiotherapy. Combined with multimodal image fusion technology, adjustment strategies after induction chemotherapy, and the forefront of future adaptive and intelligent radiotherapy, it provides reference for the formulation of clinical treatment plans and standardized target tumor delineation.
Target delineation in the era of 2D-RT
In the era of 2D-RT, radiotherapy plans are mainly based on anteroposterior and lateral X-ray images, and the treatment field setting heavily relies on anatomical experience and traditional standards [12]. The irradiation range of the primary lesion of NPC usually includes: upper boundary: the upper edge of the sella turcica or the base of the frontal sinus; lower bound: level of hyoid bone or cricoid cartilage; front boundary: posterior wall of nasal cavity; posterior boundary: the first cervical vertebra or slope [13]. Cervical lymphatic irradiation usually uses contralateral or three fields, covering the I-V area, with an irradiation range from the skull base to the supraclavicular fossa [14], without clear imaging support.
NPC patients had relatively low local control and survival rates due to technological limitations in the early era of 2D-RT. A retrospective study in Hong Kong analyzed NPC patients (n = 2687) who received radiotherapy from 1996 to 2000. Among them, 90% of patients received 2D-RT. It was found that their 5-year overall survival (OS) rate was only 75%, and the local recurrence rate was as high as 15% or more, especially in T3-T4 stage patients [15]. A study on the coverage of NPC target area by 2D-RT showed a 5-year local recurrence free rate (LRFS) of 66%. The gross tumor volume (GTV) was covered by 95% isodose lines in only 9% of patients [14]. Another study from Hong Kong showed that under a 2D-RT regimen, the average maximum doses to the brainstem and spinal cord were 61.8 Gy and 56 Gy, respectively, both exceeding the conventional dose limits of 54 Gy for the brainstem and 45 Gy for the spinal cord [16]. Over-irradiation of normal tissues may result in significant toxicity burden. These data provide a realistic foundation and comparative background for the subsequent application of 3D technology and IMRT.
Challenges in the 2D-RT era include blurred target boundaries, inaccurate tumor delineation leading to under- or overexposure, and significant radiation toxicity to normal tissues like the brainstem, cochlea, and spinal cord. Additionally, 2D-RT fails to account for tumor heterogeneity and individual anatomical variations.
3D-CRT and IMRT
The popularization of CT simulation positioning has led radiotherapy from empirical field setting to image-guided approach [17]. Through 3D reconstruction, physicians can identify tumor boundaries and draw accurate GTV. This stage marks the introduction of the concepts of CTV (clinical target volume) and PTV (planning target volume), and the shift of radiotherapy dose from a single plane to volume control.
IMRT regulates the shape and intensity of the radiation beam through a multi-directional multi leaf collimator, achieving "dose carving" while balancing high-dose tumor coverage and organs at risk (OAR) [18]. RTOG 0225 and 0615 studies constructed a standard target area stratification for NPC: GTVnx: visible portion of primary lesion image; GTVnd: lymph node metastasis with clear imaging; CTV1 (high-risk area): GTVnx extends 5-10 mm, covering the pharyngeal opening of the Eustachian tube, posterior nasal orifice, upper edge of the hard palate, and so on; CTV2 (medium low risk area): II-IV and other lymphatic drainage areas, with lower doses (54-60 Gy) [19, 20]. This scheme has become a classic reference for IMRT target delineation.
IMRT greatly improves the treatment efficacy of NPC. A retrospective study of 847 NPC patients treated with IMRT radiotherapy showed a 5-year LRFS rate of 94.3% [21], far superior to historical 2D-RT data. Additionally, a multicenter study involving 22,302 NPC patients found a 2.68% incidence of radiation-induced cranial nerve paralysis and a median survival of 13.2 years, confirming IMRT's safety and effectiveness [22]. Massachusetts General Hospital has proposed an individualized CTV delineation scheme for NPC, which involves reducing the target area, including only delineating the ipsilateral pharyngeal space, irregularly including the nasal/maxillary sinus or ethmoid sinus, not delineating the pharyngeal airway, and irregularly delineating the sphenoid sinus. The 5-year local control rate was 94%, and all four patients who experienced local recurrence were GTV intratumoral recurrence [23]. Their results indicate that narrowing the target area can achieve good local control, minimal toxic reactions, and no field recurrence. State Key Laboratory of Oncology in Southern China conducted MRI monitoring of local progression patterns in 943 NPC patients, and developed a new personalized CTV plan based on the results: CTV1 is GTV external placement of 5-10mm, including the entire nasopharyngeal mucosa and pharyngeal fascia structure; CTV2 includes all bilateral high-risk areas (parapharyngeal space, posterior nasal cavity, pterygoid process, anterior vertebral muscles, clitoris, petrous apex, hiatus, base of sphenoid bone) [24]. Sun Yat-sen University Cancer Center has refined the CTV delineation plan for early NPC T1 and T2 staging, reduced the range of CTV, decreased the radiation dose, and adopted an accelerated large segment radiotherapy plan (GTVp: 68Gy/30F). Follow up for 10 years showed that this plan achieved high local control rate and overall survival rate [25]. For patients with unilateral NPC without contralateral posterior pharyngeal lymph node metastasis or EBV-DNA positivity, studies have shown that CTV range can be reduced (reducing the contralateral posterior upper wall, but including the contralateral pharyngeal recess) [26]. Cancer Hospital of Fujian Medical University analyzed 414 cases of "small target area CTV" scheme, and found that the boundary distance of GTV-CTV2 in locally advanced (T3, T4) patients was smaller compared to the average level of all patients, but the local control rate of the tumor did not significantly decrease. A new CTV target area delineation approach was proposed: CTV = GTV + certain external edges + entire nasopharyngeal mucosa [27]. The research results on the application of improved reduced IMRT in NPC showed that abandoning CTV1 and reducing CTV2 from the 10mm edge of GTV to 8mm resulted in a 4-year local control rate of 96.6% [28]. Table 1 presents 15 studies from multiple countries and regions, covering 5-year overall survival (OS) of NPC under different technical pathways such as 2D-RT, 3D-RT, IMRT, volumetric modulated arc therapy (VMAT), and proton radiotherapy, reflecting the improvement of prognosis with advances in treatment technology [14, 15, 29-41].
Comparison of 5-year OS of NPC patients under different periods and techniques.
| Radiotherapy techniques | Author, Year | Case | 5-year OS | Note |
|---|---|---|---|---|
| 2D-RT | Waldron et al., 2003 [14] | 94 | 88% | The Princess Margaret Hospital, 1993-1997 |
| 2D-RT | Lee et al., 2005 [15] | 1282 | 62% | Hong Kong, 1980-1995 |
| 2D-RT+CCRT | Wei et al., 1998 [29] | 298 | 63.4% | Cisplatin synchronous chemotherapy |
| 3D-CRT | Tang et al., 2006 [30] | 87 | 88.2% (3-year OS) | State Key Laboratory of Oncology in South China, 2001-2004 |
| 3D-CRT | Yi et al., 2006 [31] | 905 | 76.1% | Beijing, 1990-1999 |
| IMRT | Kam et al., 2007 [32] | 193 | 83% | The Chinese University of Hong Kong, forward-looking |
| IMRT | Su et al., 2012 [33] | 198 | 97.3% | 2001-2008, patients in stages T1-T2 |
| IMRT | Lee et al., 2009 [34] | 74 | 85% | MSKCC, USA |
| IMRT ± CCRT | Yi et al., 2014 [35] | 333 | 79.4% | locoregionally advanced NPC, 2001-2009 |
| IMRT + CCRT | Chen et al., 2013 [36] | 508 | 84.0% | Sun Yat-sen University Cancer Centre, patients in non-metastatic stage III or IV (except T3-4N0) |
| IMRT + IC + CCRT | Sun et al., 2016 [37] | 480 | 90% | RCT, patients in stage III-IVB (except T3-4N0) |
| IMRT + IC + CCRT | Zhang et al., 2020 [38] | 541 | 89.5% | Tiggio/paclitaxel induction regimen |
| VMAT + IC | Liu et al., 2018 [39] | 139 | 57.5% | patients in stage II-IVB |
| IMPT | Lewis et al., 2016 [40] | 10 | 88.9% (2-year OS) | MD Anderson Cancer Center |
| IMPT | Li et al., 2021 [41] | 77 | 100% (3-year OS) | Memorial Sloan Kettering Cancer Center |
OS: overall survival; NPC: nasopharyngeal carcinoma; 2D-RT: two-dimensional radiotherapy; 3D-CRT: three-dimensional conformal radiotherapy; IMPT: intensity modulated proton therapy
Fine delineation of target area guided by MRI and PET-CT
The superior soft tissue resolution of MRI has unique value in evaluating skull base bone destruction, cavernous sinus, and temporal lobe invasion. MRI/CT fusion has become the standard technique for GTVnx delineation [42]. PET-CT can be used to identify metabolically active lymph nodes without significant enlargement on imaging, which helps to confirm the GTVnd boundary and reduce the risk of missed or overexploited target areas [43, 44]. At present, it is recommended to combine MRI (structure) + CT (dose planning) + PET (metabolism) three modes to improve the accuracy of target areas.
Ng et al. [45] analyzed the value of MRI/CT fusion in tumor delineation and found that the fusion group had an average reduction of 18% in GTV volume in the posterior wall of the nasopharynx, skull base, and other areas compared to the CT group alone, and the recurrence rate also decreased. In terms of PET/CT, Leung TW et al. [46] found that 38% of patients with PET positive but CT negative lymph nodes developed regional recurrence during follow-up, suggesting that PET can identify potential lesions in advance and improve the sensitivity of GTVnd delineation. PET/MRI has advantages in anatomical resolution and metabolic activity identification of target area delineation, especially suitable for evaluation after induction chemotherapy [47].
Standardization and optimization of target area delineation in the cervical lymphatic region
The Robbins system proposed the subdivision of cervical lymphatic regions into zones I-VII in 2003. The 2013 DAHANCA guidelines provided CT axial anatomical boundaries, becoming the most widely used reference currently [48]. Lymph node metastasis in NPC is most common in region II (> 80%), followed by regions III and IV, and rare in regions I and VI [49]. According to this mode, selective irradiation of the radiotherapy target area is feasible, avoiding full neck irradiation.
Multiple studies [50-54] have supported the safety and efficacy of selective cervical lymphatic irradiation in low-risk populations of NPC from different perspectives (Table 2). Tang LL et al. [50] published a nationwide multicenter randomized controlled study, which showed no statistically significant difference in 5-year regional control rate between irradiation of only the upper cervical lymph zone (II-IV zone) and traditional whole neck irradiation (95.7% vs 96.3%, P = 0.73), while adverse reactions such as difficulty swallowing and dry mouth significantly decreased. In addition, Hu et al. [52] omitted contralateral lower neck irradiation for 52 N1 patients. The results showed that only one patient experienced neck recurrence in the irradiated area, while no patient experienced lymph node recurrence outside the field. Cao et al. [55] evaluated the local mass and lymph node metastasis of NPC patients based on PET/MR, and found that only 1.9% of patients experienced skipping lymph node metastasis. The jumping pattern of lymph node metastasis is not common, and participatory radiotherapy may be feasible for cervical lymph node and VIIb levels below the tail edge of the cricoid cartilage. Therefore, selective irradiation is not only safe, but also beneficial for reducing treatment burden and improving QoL, especially for early or low load patients. These studies have suggested that in the population of stages N0-N1 and T1-T3, only irradiation of zones II-IV or II-III can achieve regional control rates similar to full neck irradiation, and selective irradiation is safe and feasible. The toxicity has significantly decreased, with a reduction in the incidence of severe dry mouth, swallowing difficulties, and hearing loss, improving the QoL. Of course, image-based MRI/PET-CT guided assessment of risk areas is the foundation for ensuring the safety of selective irradiation. In the era of whole neck CT, whole neck MRI, PET-CT, it is not necessary to perform long-distance lymphatic irradiation.
Selective Neck Lymphatic Region Radiation vs. Whole Neck Radiation.
| Author (year) | Stage | Groups | 5-year regional control rate | Grade III dry mouth rate | Conclusion |
|---|---|---|---|---|---|
| Tang LL et al., 2022 [50] | N0-N1 | II-IV vs whole neck | 95.7% vs 96.3% | 9.4% vs 18.2% | RCT, Selective irradiation does not reduce control rate |
| Seol KH et al., 2016 [51] | T1-4N0-3M0 | level Ib, IV, and Vb nodes omitted | 87.1% (3-year) | - | No nodal failure |
| Hu W et al., 2013 [52] | N1 | contralateral lower neck omitted | 94.3% (3-year) | - | Omitted the contralateral lower neck in a N1 stage NPC was safe and practicable |
| Li JG et al., 2013 [53] | T1-4N0M0 | upper neck irradiation vs. whole neck irradiation | 89.8% vs 89.3%(3-year) | 1.3%vs 2.7% | Prophylactic upper neck irradiation is sufficient for patients with node-negative NPC |
| Chen JZ et al., 2013 [54] | T1-4N0-1M0 | elective neck irradiation to level IV and Vb nodes | 95.6% | 17.9% (> Grade II) | Elective neck irradiation to level IV and Vb nodes in N0-1 NPC is safe |
Target delineation strategy after induction chemotherapy
Chemotherapy regimens such as gemcitabine plus cisplatin (GP) and paclitaxel plus cisplatin (TP) can reduce GTV and clear micro metastases [56]. Yang et al. [11] compared in a prospective clinical trial whether reducing the target volume of IMRT after induction chemotherapy (IC) would affect local control and survival rate. The results showed that reducing the IMRT target volume after IC did not decrease the local control rate and survival rate of locally advanced NPC, but the dose received by normal tissues decreased and the QoL score improved. A prospective phase II study showed that reducing the target volume dose after NPC induced chemotherapy can achieve good local control, limited marginal and field recurrence, and mild late toxicity. Compared with before IC, the target volume after IC significantly decreased, especially for GTVnx and GTVnd [57]. A prospective randomized multicenter study showed that reducing the IMRT target area after IC does not affect the local control and survival rate of NPC patients, and can improve their QoL [11]. A total of 57 NPC patients underwent IC+CCRT to delineate residual tumor volume as GTV and a radiation dose of 60 Gy. The results showed that the five-year overall survival rate, local recurrence free, distant metastasis free, and progression free survival rates were 82.2%, 85.8%, 87.7%, and 80.3%, respectively [58]. A randomized, noninferiority, multicenter phase III clinical study comparing the efficacy of reduced volume (tumor volume after chemotherapy) and traditional volume (tumor volume before chemotherapy) radiotherapy. The results showed that the 3-year local recurrence free survival rate was similar between the two groups (91.5% vs 91.2%). There was no significant difference in FFS, OS, and DMFS. The reduced-volume radiotherapy group showed a significant decrease in both acute and late radiotherapy-related toxicity, along with a notable improvement in QoL [59]. The study made the following adjustments to target area delineation: 1) For posterior nasal invasion regression, GTV was delineated based on pre-induction chemotherapy MRI to include the left posterior nasal cavity, and post-chemotherapy MRI excluded the left posterior nostril. 2) For cervical lymph node regression, GTV included the entire level II region on pre-induction chemotherapy MRI, and only residual lymph nodes were included on post-chemotherapy MRI. 3) GTV delineation for skull base bone invasion was based on pre-chemotherapy MRI. 4) Tumor regression areas induced by chemotherapy were included in CTV1. Furthermore, according to the expert consensus published in 2025, for GTVnd with complete remission after IC, dose reduction or narrowing of CTV range can be considered, and it is recommended to combine PET-CT and MRI for accurate evaluation [60]. Is the reduction of the primary lesion still based on pre-IC imaging? Does GTVnd disappearance require full dose irradiation? The international consensus of 2025 [60] suggests that GTVnx and GTVnd should still be based on IC; After confirming complete remission through PET-CT combined with IC, the CTV1 range can be appropriately reduced. It can be seen that both domestic and foreign experts believe that the delineation of NPC target areas after IC can narrow down the scope, but there is still some controversy over the specific scope of narrowing, which requires us to conduct more large-scale research.
Adaptive Radiation Therapy (ART)
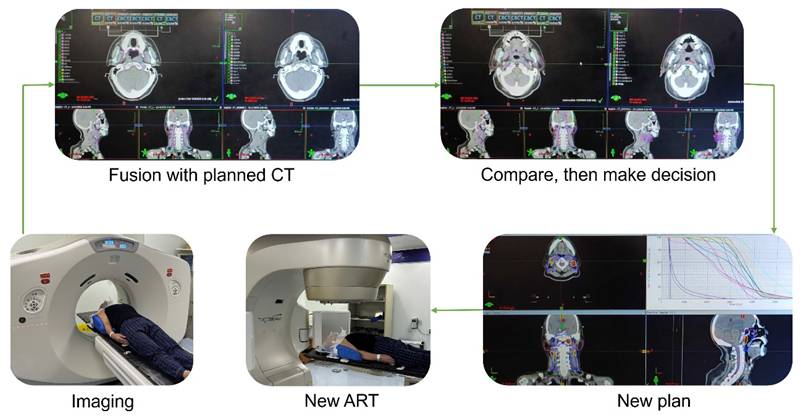
ART allows for reassessment of target area volume and morphology during treatment (such as tumor shrinkage, weight loss), re planning based on repositioning CT or MRI, reducing toxic side effects, and maintaining target area coverage [61]. Daily Cone Beam Computed Tomography (CBCT) positioning can identify changes in body position and volume reduction, which helps ensure treatment accuracy [62]. The process of ART is shown in Figure 1. Firstly, CT, MRI, or CBCT images are used, and then the obtained images are fused and registered with the previous planned CT to evaluate the position and dose errors of the target area and OARs, and then, determine whether ART is needed. If the positional deviation is significant, target area correction and plan adjustment will be carried out, and finally a new plan will be used for treatment.
The process of ART. As indicated by the arrow, the first step is to obtain the image; Match the acquired images with the planned CT images; Evaluate the position and dose errors of the target area and OAR, and determine whether ART is needed; If ART is required, readjust the target area and OAR on a new CT to generate a new radiotherapy plan; Finally, use the new plan for treatment.
The clinical research on ART in the treatment of head and neck malignant tumors continues to accumulate, showing that it can improve dose consistency and reduce toxic reactions. Zhao et al. [63] analyzed 33 NPC patients and found that ART reprogramming improved the 3-year local progression free survival rate of patients with AJCC stage T (3,4) N (x) and alleviated late-stage adverse reactions in patients with large lymph nodes [AJCC stage T (x) N (2,3)]. The head and neck tumor ART study conducted by Bhide SA et al. [64] in the UK found that weekly CT monitoring and re planning can reduce the dose to the posterior pharyngeal wall and parotid gland by up to 23%, and improve PTV consistency by 8%. ART is an effective method to improve the precision of radiotherapy implementation. One offline replanning can optimize target coverage, reduce OARs dose, improve tumor control rate, and enhance long-term QoL. ART has shown great potential in NPC, and in the future, combining automatic delineation with artificial intelligence may further improve efficiency and individualization levels.
Future direction
Using artificial intelligence (AI) and radiomics to assist in target area delineation is expected to achieve better grained individual planning. Combining PET/CT, MRI spectra, metabolic maps, and molecular markers can further enhance the biological accuracy of target area definition. AI can automatically outline and adapt formulaic target areas, reducing manual effort and standardizing the process. Several studies have developed automatic delineation models based on deep learning [65-67], significantly improving the efficiency and consistency of NPC delineation. Imaging omics can predict the risk of local recurrence in advance and provide scientific basis for individualized ART plans [68]. Multiple studies have reviewed the systematic application of AI in online re planning, target area prediction, and normal tissue protection, providing a technical blueprint for the development direction of AI driven ART [9, 69, 70].
Conclusions
The delineation of NPC target areas has evolved from two-dimensional empirical field setting to precise individualized planning based on multimodal imaging. The target area regulation after induction chemotherapy, the rise of ART, and the introduction of AI technology will further promote the intelligence and precision of NPC radiotherapy. The future target area definition should integrate multidimensional information such as imaging, molecular markers, and immune responses to achieve a new pattern of radiotherapy that is "precise definition, individual regulation, and real-time adaptation".
Author Contributions
Xiaojing Yang: Writing - review & editing; Lijun Liu: Imaging; Huicai Zhang: Imaging; Hanru Ren: Tabulating and auditing; Jie Fu: Writing - review & editing.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Luo W. Nasopharyngeal carcinoma ecology theory: cancer as multidimensional spatiotemporal "unity of ecology and evolution" pathological ecosystem. Theranostics. 2023;13(5):1607-31
2. Chang ET, Ye W, Zeng YX, Adami HO. The Evolving Epidemiology of Nasopharyngeal Carcinoma. Cancer Epidemiol Biomarkers Prev. 2021;30(6):1035-47
3. Wong KCW, Hui EP, Lo KW. et al. Nasopharyngeal carcinoma: an evolving paradigm. Nat Rev Clin Oncol. 2021;18(11):679-95
4. Tang LL, Guo R, Zhang N. et al. Effect of Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients With Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial. JAMA. 2022;328(8):728-36
5. Yang X, Ren H, Li Z, Peng X, Fu J. Combinations of radiotherapy with immunotherapy in nasopharyngeal carcinoma. Int Immunopharmacol. 2023;125(Pt A):111094
6. Wang X, Huang N, Yip PL. et al. The individualized delineation of clinical target volume for primary nasopharyngeal carcinoma based on invasion risk of substructures: A prospective, real-world study with a large population. Radiother Oncol. 2024;194:110154
7. Dang H, Zhang J, Wang R. et al. Glioblastoma Recurrence Versus Radiotherapy Injury: Combined Model of Diffusion Kurtosis Imaging and 11C-MET Using PET/MRI May Increase Accuracy of Differentiation. Clin Nucl Med. 2022;47(6):e428-e36
8. Thureau S, Briens A, Decazes P. et al. PET and MRI guided adaptive radiotherapy: Rational, feasibility and benefit. Cancer Radiother. 2020;24(6-7):635-44
9. Dona Lemus OM, Cao M, Cai B, Cummings M, Zheng D. Adaptive Radiotherapy: Next-Generation Radiotherapy. Cancers (Basel). 2024 16(6)
10. Xiang L, Rong JF, Xin C. et al. Reducing Target Volumes of Intensity Modulated Radiation Therapy After Induction Chemotherapy in Locoregionally Advanced Nasopharyngeal Carcinoma: Long-Term Results of a Prospective, Multicenter, Randomized Trial. Int J Radiat Oncol Biol Phys. 2023;117(4):914-24
11. Yang H, Chen X, Lin S. et al. Treatment outcomes after reduction of the target volume of intensity-modulated radiotherapy following induction chemotherapy in patients with locoregionally advanced nasopharyngeal carcinoma: A prospective, multi-center, randomized clinical trial. Radiother Oncol. 2018;126(1):37-42
12. Teo PM, Ma BB, Chan AT. Radiotherapy for nasopharyngeal carcinoma-transition from two-dimensional to three-dimensional methods. Radiother Oncol. 2004;73(2):163-72
13. Mao YP, Zhou GQ, Liu LZ. et al. Comparison of radiological and clinical features of temporal lobe necrosis in nasopharyngeal carcinoma patients treated with 2D radiotherapy or intensity-modulated radiotherapy. Br J Cancer. 2014;110(11):2633-9
14. Waldron J, Tin MM, Keller A. et al. Limitation of conventional two dimensional radiation therapy planning in nasopharyngeal carcinoma. Radiother Oncol. 2003;68(2):153-61
15. Lee AW, Sze WM, Au JS. et al. Treatment results for nasopharyngeal carcinoma in the modern era: the Hong Kong experience. Int J Radiat Oncol Biol Phys. 2005;61(4):1107-16
16. Chau RM, Teo PM, Kam MK, Leung SF, Cheung KY, Chan AT. Dosimetric comparison between 2-dimensional radiation therapy and intensity modulated radiation therapy in treatment of advanced T-stage nasopharyngeal carcinoma: to treat less or more in the planning organ-at-risk volume of the brainstem and spinal cord. Med Dosim. 2007;32(4):263-70
17. Li H, Yu L, Anastasio MA. et al. Automatic CT simulation optimization for radiation therapy: A general strategy. Med Phys. 2014;41(3):031913
18. Nakamura N, Shikama N, Oguchi M. [Intensity-modulated radiation therapy (IMRT)]. Nihon Rinsho. 2010;68(6):1035-9
19. Qian J, Yang Y, Xing P, Wang C, Tian Y, Lu X. Differences in lower cranial nerve complications predicted by the NTCP model between RTOG and reduced-volume IMRT planning in radiotherapy for nasopharyngeal carcinoma. Transl Cancer Res. 2020;9(1):300-8
20. Liang SB, Wang Y, Hu XF. et al. Survival and Toxicities of IMRT Based on the RTOG Protocols in Patients with Nasopharyngeal Carcinoma from the Endemic Regions of China. J Cancer. 2017;8(18):3718-24
21. Yin WJ, Mao W, Yang F. et al. Effect analysis of 847 nasopharyngeal carcinoma cases treated with intensity modulated radiation: Experience and suggestions. Oral Oncol. 2024;158:107001
22. Pan T, Li X, Zhao B. et al. Radiotherapy-Related Neurologic Complications in Patients with Nasopharyngeal Carcinoma: A Multicenter Epidemiologic Study in Southern China. Cancer Epidemiol Biomarkers Prev. 2022;31(5):1119-29
23. Sanford NN, Lau J, Lam MB. et al. Individualization of Clinical Target Volume Delineation Based on Stepwise Spread of Nasopharyngeal Carcinoma: Outcome of More Than a Decade of Clinical Experience. Int J Radiat Oncol Biol Phys. 2019;103(3):654-68
24. Liang SB, Sun Y, Liu LZ. et al. Extension of local disease in nasopharyngeal carcinoma detected by magnetic resonance imaging: improvement of clinical target volume delineation. Int J Radiat Oncol Biol Phys. 2009;75(3):742-50
25. Miao J, Di M, Chen B. et al. A Prospective 10-Year Observational Study of Reduction of Radiation Therapy Clinical Target Volume and Dose in Early-Stage Nasopharyngeal Carcinoma. Int J Radiat Oncol Biol Phys. 2020;107(4):672-82
26. Li AC, Zhang YY, Zhang C, Wang DS, Xu BH. Pathologic study of tumour extension for clinically localized unilateral nasopharyngeal carcinoma: Should the contralateral side be included in the clinical target volume? J Med Imaging Radiat Oncol. 2018
27. Lin S, Pan J, Han L. et al. Update report of nasopharyngeal carcinoma treated with reduced-volume intensity-modulated radiation therapy and hypothesis of the optimal margin. Radiother Oncol. 2014;110(3):385-9
28. Guo Q, Zheng Y, Lin J. et al. Modified reduced-volume intensity-modulated radiation therapy in non-metastatic nasopharyngeal carcinoma: A prospective observation series. Radiother Oncol. 2021;156:251-7
29. Wei WI, Sham JS. Nasopharyngeal carcinoma. Lancet. 2005;365(9476):2041-54
30. Tang YQ, Luo W, He ZC, Sun Y, Lu TX. [Three-dimensional conformal radiotherapy for primary nasopharyngeal carcinoma and analysis of locoregional recurrence]. Ai Zheng. 2006;25(3):330-4
31. Yi JL, Gao L, Huang XD. et al. Nasopharyngeal carcinoma treated by radical radiotherapy alone: Ten-year experience of a single institution. Int J Radiat Oncol Biol Phys. 2006;65(1):161-8
32. Kam MK, Leung SF, Zee B. et al. Prospective randomized study of intensity-modulated radiotherapy on salivary gland function in early-stage nasopharyngeal carcinoma patients. J Clin Oncol. 2007;25(31):4873-9
33. Su SF, Han F, Zhao C. et al. Long-term outcomes of early-stage nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy alone. Int J Radiat Oncol Biol Phys. 2012;82(1):327-33
34. Lee N, Xia P, Quivey JM. et al. Intensity-modulated radiotherapy in the treatment of nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat Oncol Biol Phys. 2002;53(1):12-22
35. Yi J, Huang X, Gao L. et al. Intensity-modulated radiotherapy with simultaneous integrated boost for locoregionally advanced nasopharyngeal carcinoma. Radiat Oncol. 2014;9:56
36. Chen L, Hu CS, Chen XZ. et al. Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2012;13(2):163-71
37. Sun Y, Li WF, Chen NY. et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016;17(11):1509-20
38. Zhang Y, Chen L, Hu GQ. et al. Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. N Engl J Med. 2019;381(12):1124-35
39. Liu L, Fei Z, Chen M. et al. Induction chemotherapy plus concurrent chemoradiotherapy versus induction chemotherapy plus volumetric modulated arc therapy alone in the treatment of stage II-IVB nasopharyngeal carcinoma patients: a retrospective controlled study. Radiat Oncol. 2018;13(1):148
40. Lewis GD, Holliday EB, Kocak-Uzel E. et al. Intensity-modulated proton therapy for nasopharyngeal carcinoma: Decreased radiation dose to normal structures and encouraging clinical outcomes. Head Neck. 2016;38(Suppl 1):E1886-95
41. Li X, Kitpanit S, Lee A. et al. Toxicity Profiles and Survival Outcomes Among Patients With Nonmetastatic Nasopharyngeal Carcinoma Treated With Intensity-Modulated Proton Therapy vs Intensity-Modulated Radiation Therapy. JAMA Netw Open. 2021;4(6):e2113205
42. Nishioka T, Shiga T, Shirato H. et al. Image fusion between 18FDG-PET and MRI/CT for radiotherapy planning of oropharyngeal and nasopharyngeal carcinomas. Int J Radiat Oncol Biol Phys. 2002;53(4):1051-7
43. Shen G, Zhang W, Jia Z, Li J, Wang Q, Deng H. Meta-analysis of diagnostic value of 18F-FDG PET or PET/CT for detecting lymph node and distant metastases in patients with nasopharyngeal carcinoma. Br J Radiol. 2014;87(1044):20140296
44. Zhang Y, Hu Y, Zhao S, Huang R. The Utility of (18)F-FDG-PET-CT Metabolic Parameters in Evaluating the Primary Tumor Aggressiveness and Lymph Node Metastasis of Nasopharyngeal Carcinoma. Clin Med Insights Oncol. 2024;18:11795549231225419
45. Ng WL, Brunt J, Temple S. et al. Volumetric modulated arc therapy in prostate cancer patients with metallic hip prostheses in a UK centre. Rep Pract Oncol Radiother. 2015;20(4):273-7
46. Leung SW, Lee TF. Treatment of nasopharyngeal carcinoma by tomotherapy: five-year experience. Radiat Oncol. 2013;8:107
47. Wong KH, Panek R, Welsh L. et al. The Predictive Value of Early Assessment After 1 Cycle of Induction Chemotherapy with 18F-FDG PET/CT and Diffusion-Weighted MRI for Response to Radical Chemoradiotherapy in Head and Neck Squamous Cell Carcinoma. J Nucl Med. 2016;57(12):1843-50
48. Zukauskaite R, Kristensen MH, Eriksen JG. et al. Comparison of 3-year local control using DAHANCA radiotherapy guidelines before and after implementation of five millimetres geometrical GTV to high-dose CTV margin. Radiother Oncol. 2024;196:110284
49. Ho FC, Tham IW, Earnest A, Lee KM, Lu JJ. Patterns of regional lymph node metastasis of nasopharyngeal carcinoma: a meta-analysis of clinical evidence. BMC Cancer. 2012;12:98
50. Tang LL, Huang CL, Zhang N. et al. Elective upper-neck versus whole-neck irradiation of the uninvolved neck in patients with nasopharyngeal carcinoma: an open-label, non-inferiority, multicentre, randomised phase 3 trial. Lancet Oncol. 2022;23(4):479-90
51. Seol KH, Lee JE. Patterns of failure after the reduced volume approach for elective nodal irradiation in nasopharyngeal carcinoma. Radiat Oncol J. 2016;34(1):10-7
52. Hu W, Zhu G, Guan X, Wang X, Hu C. The feasibility of omitting irradiation to the contralateral lower neck in stage N1 nasopharyngeal carcinoma patients. Radiat Oncol. 2013;8:230
53. Li JG, Yuan X, Zhang LL. et al. A randomized clinical trial comparing prophylactic upper versus whole-neck irradiation in the treatment of patients with node-negative nasopharyngeal carcinoma. Cancer. 2013;119(17):3170-6
54. Chen JZ, Le QT, Han F. et al. Results of a phase 2 study examining the effects of omitting elective neck irradiation to nodal levels IV and Vb in patients with N(0-1) nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2013;85(4):929-34
55. Cao C, Xu Y, Huang S. et al. Locoregional Extension Patterns of Nasopharyngeal Carcinoma Detected by FDG PET/MR. Front Oncol. 2021;11:763114
56. Lian CL, Zhou R, Zhou Y, Zhou P, Wu SG. Assessment of Response to Different Induction Chemotherapy Regimens in Locally Advanced Nasopharyngeal Carcinoma. Drug Des Devel Ther. 2023;17:551-62
57. Zhao C, Miao JJ, Hua YJ. et al. Locoregional Control and Mild Late Toxicity After Reducing Target Volumes and Radiation Doses in Patients With Locoregionally Advanced Nasopharyngeal Carcinoma Treated With Induction Chemotherapy (IC) Followed by Concurrent Chemoradiotherapy: 10-Year Results of a Phase 2 Study. Int J Radiat Oncol Biol Phys. 2019;104(4):836-44
58. Wang L, Wu Z, Xie D. et al. Reduction of Target Volume and the Corresponding Dose for the Tumor Regression Field after Induction Chemotherapy in Locoregionally Advanced Nasopharyngeal Carcinoma. Cancer Res Treat. 2019;51(2):685-95
59. Tang LL, Chen L, Xu GQ. et al. Reduced-volume radiotherapy versus conventional-volume radiotherapy after induction chemotherapy in nasopharyngeal carcinoma: An open-label, noninferiority, multicenter, randomized phase 3 trial. CA Cancer J Clin. 2025;75(3):203-15
60. Fourati N, Bacorro W, Nouri O. et al. International Consensus Guidelines on the Delineation of Radiation Therapy Target Volumes for Nasopharyngeal Carcinoma After Induction Chemotherapy Using a 2-Round Modified Delphi Survey. Pract Radiat Oncol. 2025;15(4):347-66
61. Lavrova E, Garrett MD, Wang YF. et al. Adaptive Radiation Therapy: A Review of CT-based Techniques. Radiol Imaging Cancer. 2023;5(4):e230011
62. Lemus OMD, Tanny S, Cummings M. et al. Influence of air mapping errors on the dosimetric accuracy of prostate CBCT-guided online adaptive radiation therapy. J Appl Clin Med Phys. 2023;24(10):e14057
63. Zhao L, Wan Q, Zhou Y, Deng X, Xie C, Wu S. The role of replanning in fractionated intensity modulated radiotherapy for nasopharyngeal carcinoma. Radiother Oncol. 2011;98(1):23-7
64. Bhide SA, Davies M, Burke K. et al. Weekly volume and dosimetric changes during chemoradiotherapy with intensity-modulated radiation therapy for head and neck cancer: a prospective observational study. Int J Radiat Oncol Biol Phys. 2010;76(5):1360-8
65. He Y, Zhang S, Luo Y. et al. Quantitative Comparisons of Deep-learning-based and Atlas-based Auto- segmentation of the Intermediate Risk Clinical Target Volume for Nasopharyngeal Carcinoma. Curr Med Imaging. 2022;18(3):335-45
66. Xue X, Qin N, Hao X. et al. Sequential and Iterative Auto-Segmentation of High-Risk Clinical Target Volume for Radiotherapy of Nasopharyngeal Carcinoma in Planning CT Images. Front Oncol. 2020;10:1134
67. Peng Y, Liu Y, Shen G. et al. Improved accuracy of auto-segmentation of organs at risk in radiotherapy planning for nasopharyngeal carcinoma based on fully convolutional neural network deep learning. Oral Oncol. 2023;136:106261
68. Bang C, Bernard G, Le WT, Lalonde A, Kadoury S, Bahig H. Artificial intelligence to predict outcomes of head and neck radiotherapy. Clin Transl Radiat Oncol. 2023;39:100590
69. Landry G, Kurz C, Traverso A. The role of artificial intelligence in radiotherapy clinical practice. BJR Open. 2023;5(1):20230030
70. Mastella E, Calderoni F, Manco L. et al. A systematic review of the role of artificial intelligence in automating computed tomography-based adaptive radiotherapy for head and neck cancer. Phys Imaging Radiat Oncol. 2025;33:100731
Author contact
![]() Corresponding authors: Hanru Ren M.D., Email: renhanru1com; Jie Fu Ph.D., Email: fujie74edu.cn.
Corresponding authors: Hanru Ren M.D., Email: renhanru1com; Jie Fu Ph.D., Email: fujie74edu.cn.