Impact Factor ISSN: 1837-9664

 Global reach, higher impact
Global reach, higher impactJ Cancer 2019; 10(6):1496-1502. doi:10.7150/jca.29595 This issue Cite
Research Paper
Current Treatment for Low-Risk Prostate Cancer in China: A National Network Survey
Yongbao Wei1,2, Longfei Liu3 ![]() , Xin Li4, Wei Song5, Dewen Zhong6, Xiande Cao7, Daozhang Yuan8, Shaoxiong Ming9, Peng Zhang10, Yanlin Wen11, Jiu Jing Group12
, Xin Li4, Wei Song5, Dewen Zhong6, Xiande Cao7, Daozhang Yuan8, Shaoxiong Ming9, Peng Zhang10, Yanlin Wen11, Jiu Jing Group12
1. Shengli Clinical Medical College, Fujian Medical University, Fuzhou 350001, China;
2. Department of Urology, Fujian Provincial Hospital, No.134 Dong Street, Fuzhou 350001, China;
3. Department of Urology, Xiangya Hospital, Central South University, Changsha, Hunan 410000;
4. Department of Urology, the 118th Hospital of PLA, Wenzhou, 325000;
5. Department of Urology, the Hunan Provincial People's Hospital, Changsha 410005;
6. Department of Urology, The First Affiliated Hospital of Fujian Medical University, Longyan, 364000;
7. Department of Urology, Affiliated hospital of Jining Medical University, Jining, 272000;
8. Department of Urology, Cancer Center of Guangzhou Medical University, Guangzhou, 510095;
9. Department of Urology, Changhai Hospital, The Second Military Medical University, Shanghai 200433;
10. Department of Urology, Zhongnan Hospital, Wuhan University, Wuhan, 430071;
11. Department of Urology,Nanchong Central Hosipital, Nanchong, 637000;
12. Jiujing, new medium team of Chinese Urologists, PR China.
Received 2018-8-30; Accepted 2019-1-16; Published 2019-2-23
Abstract
Objective: To analyze the current treatment for low-risk prostate cancer (LRPC) in China.
Methods: A national questionnaire survey titled “A survey of current treatment of LRPC” was designed and released nationally through the network from July 16 to August 3, 2017.
Results: A total of 1,116 valid questionnaires were recovered. The percentages of preferred treatment by active surveillance (AS) or radical prostatectomy (RP) were 29.21% and 45.61%, respectively. A correspondence analysis showed that the physician in charge was more inclined to choose AS than RP. Respondents from different institution types, hospitals with different annual numbers of newly admitted patients with prostate cancer, and with different familiarity with the LRPC definition presented a significant difference in the preferred treatments (p < 0.05). Urologists chose AS or not for the following reasons: tumor progression (52.51%), potential medical disputes (42.56%) (i.e., medical disputes from patients or their relatives when urologists choose AS to treat patients with LRPC and the patient has a poor outcome), fear of cancer (41.94%), and surgical risk (39.07%). These reasons were ubiquitous, and there was no significant difference among urologists for these concerns (p > 0.05). Personal skills, surgical risk, and tumor progression were the most common factors that influenced whether AS or RP was preferred (p < 0.05). Concern about the medical disputes brought about by AS was a key factor for not choosing AS (p < 0.05).
Conclusions: LRPC is still dominated by RP in China, followed by AS. Personal skills, surgical risk, and concern about tumor progression were the common factors influencing whether AS or RP was preferred. In addition, medical disputes brought by AS are another key factor for not choosing AS. There will be more Chinese data in the future to guide treatment of LRPC.
Keywords: prostate cancer, active surveillance, radical prostatectomy, urologist, China, survey
Introduction
All guidelines except the Chinese Urological Association(CUA), including the American Urological Association, the European Association of Urology (EAU), the Japanese Urological Association, and the Canadian Urological Association currently have clear recommendations for treating low-risk prostate cancer (LRPC). Among them, active monitoring or surveillance (AS) is the most widely advised treatment [1]. If LRPC is treated with radical prostatectomy (RP) or radiotherapy, it may be overtreated, which has no benefit to the patient and increases the complication rate[2, 3] and wastes limited medical resources, leading to delayed treatment opportunities for those who have more aggressive prostate cancer (PCa). These guidelines have greatly influenced clinical practice. The current Chinese guidelines were released in 2014 and have not been updated recently. The CUA proposes AS for patients with PCa characterized with a prostate specific antigen (PSA) < 10 ng/mL, Gleason score ≤ 6, positive number of biopsies ≤ 3, proportion of tumor in each puncture specimen ≤ 50%, and clinical stage 2a, which is similar to the generally accepted standard[4-6]. Development of the CAU guidelines depends on updates of the European and American guidelines[7]. The recommendations of multiple guidelines[8] and an increasing number of studies have demonstrated the important role of AS in LRPC[9]. We conducted this real-world nationwide survey from July 16 to August 3, 2017, based on the new we-media platform of Chinese Urologists called JIU JING to understand current treatments for LRPC in China.
Methods
We used the online questionnaire instrument WENJUANXIN (https://www.wjx.cn/#c360), which is a platform for professional online surveying, evaluation, and voting in China, to design “A survey for current treatment of LRPC”. This study was approved by the Ethics Committee of Xiangya Hospital of Central South University. It was performed from July 16 to August 3, 2017. The investigation was carried out based on the Chinese urologist's new we-media platform JIU JING to release an electronic questionnaire through WeChat software, which is a famous real-time soft chat on the China mainland. The survey was online and was released to mobile phone clients. The respondents were urologists from all over the country. Each mobile platform could be filled only once. The whole survey took 2-10 min to complete. All successful submissions were valid questionnaires, as the questionnaire must be completed before it could be submitted successfully. The survey contained 11 items, divided into three domains, including general information about the respondent, LRPC treatment choice, and an evaluation of the current treatment status and CAU guidelines. The general information included gender (item 1), title (item 2), institution type (item 3), the annual number of newly admitted patients with PCa (item 4), and familiarity with the LRPC definition (item 5). The choice of treatment included which treatments were appropriate for LRPC (item 6), the most preferred treatment (item 7), and the reasons for using AS or not (item 8). The evaluations included problems common to doctors when designing a treatment plan (item 9), problems of current PCa treatments (item 10), and an evaluation of the current 2014 CAU vision guidelines (item 11).
All data were entered, analyzed, and processed using SPSS 24.0 software Student Edition (SPSS Inc., Chicago, Il, USA). The chi-square test, a correspondence analysis, and a logistic regression analysis were performed. A p-value < 0.05 was considered significant.
Results
General information
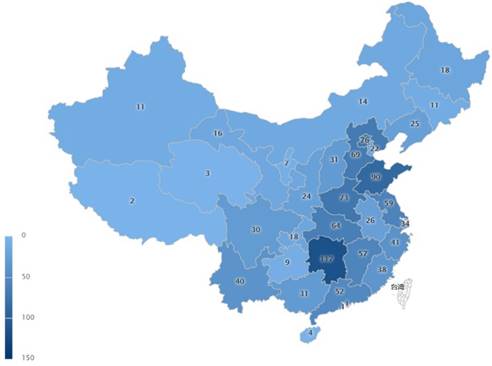
A total of 1,116 valid questionnaires [1,081 respondents (96.9%) were males and 35 (3.1%) were females] covering the entire country ( Hong Kong and Macau, except Taiwan) (Figure 1) were obtained. The average completion time was 4.5 min. The titles of the Chinese doctors were divided into the following four grades of primary physician [156 (14.0%)], physician in charge [336 (30.1%)], assistant director physician [436 (39.1%)], and director physician [188 (16.8%)]. The types of Chinese mainland hospitals in this study were divided into national or ministerial level, provincial or municipality level, city level, and level of the county and below. In this study, the numbers of respondents from the first two levels were 72 (6.5%) and 229 (20.5%), respectively. These two levels of hospitals are the most important institutions for diagnosing and treating patients with PCa. The annual numbers of newly admitted patients with PCa were divided into the following five grades: > 200 (74, 6.6%), 100-200 (113, 10.1%), 50-100 (215, 19.3%), 20-50 (329, 29.5%), and < 20 people (382, 34.5%). The definition of LRPC in the 2014 CUA guidelines is consistent with that of the EAU guidelines. Among the respondents familiar with the LRPC definitions, 20.5% (229) were very familiar, and 58.9% (657) reported familiar (Table 1).
A total of 1,116 valid questionnaires was obtained, covering the whole country, including Hong Kong and Macau, but not Taiwan.
General information of respondents
| Items | Values (n, %) | |
|---|---|---|
| Gender | Male | 1081(96.9) |
| Female | 35(3.1) | |
| Titles | Director physician | 156(14.0) |
| Assistant director physician | 336(30.1) | |
| Physician in charge | 436(39.1) | |
| Primary physician | 188(16.8) | |
| Hospital types | National or ministerial level | 72(6.5) |
| Provincial or municipality level | 229(20.5) | |
| City level | 459(41.1) | |
| Level of county and below | 356(31.9) | |
| ANP | >200 | 74(6.6) |
| 100-200 | 113(10.1) | |
| 50-100 | 215(19.3) | |
| 20-50 | 329(29.5) | |
| <20 | 385(34.5) | |
| FLD | Very familiar | 229(20.5) |
| Familiar | 657(58.9) | |
| Uncertain | 164(14.7) | |
| Unknown | 66(5.9) | |
ANP=annual numbers of newly admitted patients with PCa; FLD=familiarity with LRPC definitions
Differences in preferred treatments exist among the groups
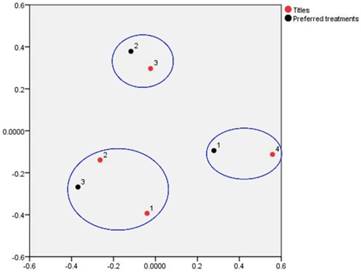
The percentages of the overall most preferred AS and RP treatments as well as other therapies were 29.2% (326), 45.6% (509), and 25.2% (281), respectively (Table 2). No significant differences in gender or title were observed between the three treatments (p > 0.05) (Table 3). A correspondence analysis was used to further analyze the choice of the preferred treatment for the different titles (Figure 2). The results in Table 2 and Figure 2 show that the urologists with different titles preferred RP, followed by AS, but physicians in charge preferred AS over RP more than the other titles. Primary physicians tended to prefer RP more than the other doctors, whereas director and assistant director physicians tended to choose “other therapies” more frequently. Significant differences exited among respondents from different institution types, hospitals with different annual numbers of newly admitted patients, and different familiarity with the LRPC definitions for the preferred treatments (p < 0.05) (Table 2). Among them, the largest proportions of respondents existed in the following groups: 50.2% (115/229) from provincial or municipality level hospitals, 54.9% (62/113) from institutions with 100-200 newly admitted patients with PCa annually, and 56.8% (130/229) who were very familiar with the LRPC definition. AS was chosen more frequently by the following groups: 36.1% (26/72) respondents from hospitals of national or ministerial level, 35.1% (26/74) from hospitals with > 200 new PCa patients annually, and 30.6% (201/657) who were familiar with the LRPC definition.
Preferred treatments and the main reasons
| Items | Values (n, %) | |
|---|---|---|
| Preferred | AS | 326(29.2) |
| treatments | RP | 509(45.6) |
| Other therapies | 281(25.2) | |
| Watchful waiting | 49(4.4) | |
| Radiotherapy | 17(1.5) | |
| ADT | 132(11.8) | |
| Local treatment | 81(7.3) | |
| Other methods | 2(0.2) | |
| Main reasons | Tumor progression | 586(52.5) |
| of whether | Medical disputes | 475(42.6) |
| choosing AS | Fear of cancer | 468(41.9) |
| Surgical risks | 436(39.1) | |
ANP=annual numbers of newly admitted patients with PCa; FLD=familiarity with LRPC definitions; AS= active surveillance; RP= radical prostatectomy; ADT=Androgen deprivation therapy
Analysis of the reasons of preferred treatments in different groups
| Items | Preferred treatments | χ2 | p | |||
|---|---|---|---|---|---|---|
| RP | AS | Other therapies | ||||
| Gender | Male | 494(45.7) | 316(29.2) | 271(25.1) | 0.23 | 0.891 |
| Female | 15(42.9) | 10(28.6) | 10(28.6) | |||
| Titles | Director physician | 73(46.8) | 39(25.0) | 96(28.2) | 10.649 | 0.100 |
| Assistant director physician | 144(42.9) | 96(28.6) | 96(28.6) | |||
| Physician in charge | 192(44.0) | 142(32.6) | 102(23.4) | |||
| Primary physician | 100(53.2) | 49(26.1) | 39(20.7) | |||
| Hospital types | National or ministerial level | 33(45.8) | 26(36.1) | 13(18.1) | 18.917 | 0.004* |
| Provincial or municipality level | 115(50.2) | 76(33.2) | 38(16.6) | |||
| City level | 207(45.1) | 133(29.0) | 119(25.9) | |||
| Level of county and below | 154(43.3) | 91(25.6) | 111(31.2) | |||
| ANP | >200 | 32(43.2) | 26(35.1) | 16(21.6) | 22.989 | 0.003* |
| 100-200 | 62(54.9) | 36(31.9) | 15(13.3) | |||
| 50-100 | 105(48.8) | 65(30.2) | 45(20.9) | |||
| 20-50 | 158(48.0) | 88(26.7) | 83(25.2) | |||
| <20 | 152(39.5) | 111(28.8) | 122(31.7) | |||
| FLD | Very familiar | 130(56.8) | 65(28.4) | 34(14.8) | 40.431 | 0.000* |
| Familiar | 295(44.9) | 201(30.6) | 161(24.5) | |||
| Uncertain | 59(36.0) | 49(29.9) | 56(34.1) | |||
| Unknown | 25(37.9) | 11(16.7) | 30(45.5) | |||
ANP=annual numbers of newly admitted patients with PCa; FLD=familiarity with LRPC definitions
A correspondence analysis was performed to analyze the preferred treatment by different physician titles. The results showed that physicians in charge preferred active surveillance (AS) more than the other titles, while primary physicians tended to prefer radical prostatectomy (RP), and director or assistant director physicians tended to prefer “other therapies” more frequently.
Analysis of the reasons for the most preferred treatments in the different groups
The reasons for choosing AS were analyzed, and the results showed that the following four factors contributed more than 30%, including 52.5% (586/1116) with concerns about tumor progression, 42.6% (475/1116) concerned about potential medical disputes, 41.9% (486/1116) fear of cancer, and 39.1% (436/1116) concern about surgical risks (Table 2). The chi-square test results revealed no significant differences in the concerns for the above four influencing factors between the genders, titles, institution types, annual numbers of newly admitted patients, and familiarity with the LRPC definition (p > 0.05). A logistic regression analysis showed that individual skills, fear of surgical risk, and tumor progression were co-influencing factors that determined whether AS or RP was preferred (p < 0.05) (Tables 3 and 4). Concern about potential medical disputes brought about by AS was a key factor for not choosing AS (p < 0.05) (Table 3).
Logistic regression analysis results of whether choosing AS
| Dependent variable | Independent variable | B | S.E. | Ostwald coefficient | p | Exp(B) | Exp(B) |
|---|---|---|---|---|---|---|---|
| 95% CI | |||||||
| AS | Genders | 0.061 | 0.398 | 0.023 | 0.879 | 1.063 | 0.487-2.318 |
| Titles | 0.048 | 0.077 | 0.396 | 0.529 | 1.05 | 0.903-1.220 | |
| Hospital types | -0.144 | 0.096 | 2.255 | 0.133 | 0.866 | 0.717-1.045 | |
| ANP | 0.017 | 0.071 | 0.056 | 0.813 | 1.017 | 0.884-1.170 | |
| FLD | -0.101 | 0.102 | 0.986 | 0.321 | 0.904 | 0.740-1.104 | |
| Individual skills | -0.563 | 0.175 | 10.388 | 0.001* | 0.57 | 0.404-0.802 | |
| Surgical risk | 0.817 | 0.142 | 33.267 | 0.000* | 2.264 | 1.715-2.989 | |
| Tumor progression | -0.334 | 0.144 | 5.386 | 0.020* | 0.716 | 0.540-0.949 | |
| Medical disputes | -0.325 | 0.156 | 4.327 | 0.038* | 0.722 | 0.532-0.981 | |
| Patient loss | 0.121 | 0.218 | 0.305 | 0.581 | 1.128 | 0.735-1.731 | |
| Fear of cancer | -0.26 | 0.15 | 2.998 | 0.083 | 0.771 | 0.574-1.035 | |
| Other reasons | 0.327 | 0.22 | 2.21 | 0.137 | 1.386 | 0.901-2.133 | |
| Constant | -0.379 | 0.521 | 0.529 | 0.467 | 0.684 | 0.487-2.318 |
ANP=annual numbers of newly admitted patients with PCa; FLD=familiarity with LRPC definitions; AS= active surveillance; CI=confidence interval
Evaluation of currently preferred treatments and current guidelines
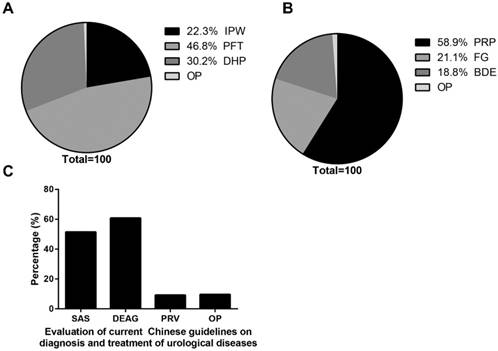
A total of 46.8% (522/1116) of the responding urologists thought that they should introduce all treatment options and let the patients choose; 30.2% (337/1116) considered that doctors should help patients choose the best treatment (Fig. 3A). The preferred PCa treatments according to the doctors were 58.9% (658/1116) considered the current bias and preferred surgery, and 21.1% (235/1116) strictly followed the PCa guidelines (Fig. 3B). Regarding evaluation of the current 2014 CUA guidelines, 60.8% (679/1116) of the physicians considered the guidelines to be relatively pertinent and they were suitable for China's actual situation; 51.4% (574/1116) believed that the guidelines lacked Chinese data, and that the guidelines were established based on the European and American guidelines (Fig. 3C). Another 9.2% (103/1116) considered that the reference value of the Chinese guidelines was weak, and they were more willing to read the European and American guidelines.
Evaluations of current preferred treatments for low-risk prostate cancer (PCa) and the current guidelines. (A) 46.8% urologists introduced all treatment options and let the patients choose themselves, followed by 30.2% considered that doctors should help patients choose the best treatment. (B) 58.9% considered the current bias and preferred surgery to treat PCa, followed by 21.1% who strictly followed the current guidelines. (C) 60.8% considered that the guidelines were relatively pertinent and suitable for China's actual situation, whereas 51.4% believed that the Chinese guidelines lacked Chinese data, and that the guidelines were established based on the European and American guidelines. Another 9.2% regarded the reference values of the Chinese guidelines as weak, and they were more willing to follow the European and American guidelines.
Discussion
AS is recommended for patients with LRPC, but AS is not the most preferred method in China. Accumulating evidence of AS for LRPC has been updated. In 2004, Cooperberg et al. concluded that LRPC had been overtreated, and that the treatment mode needed to be changed[2]. In 2015, the ASCO Endorsement Panel team recommended AS for patients with LRPC [3]. A study of 82,429 patients with localized PCa followed-up for 10 years showed no significant differences in PCa-specific mortality among AS, RP, and radiotherapy; but RP and radiotherapy reduced tumor progression and the risk of metastasis compared with AS [10]. Another study on PCa followed-up for 20 years also showed that RP does not significantly reduce all-cause mortality or tumor-specific mortality compared with AS, and RP results in associated complications[11]. Nearly 30% of patients require other treatments, such as surgery and radiotherapy, within 5 years of AS[12], but AS is still widely used and recommended for patients with LRPC [1, 8]. The 2014 edition of the CUA guidelines proposed an indication of AS for PCa confirmed by prostate biopsy, which was similar to other indications [4-6]. Although different guidelines have highlighted AS as the first line recommended treatment for LRPC[1], RP, not AS, was the first choice in China, while AS is the second most preferred. Our survey found that AS and RP were preferred for LRPC in 29.2% and 45.6% of cases, respectively. This significant difference was not observed between the different genders and titles. The correspondence analysis determined that physicians in charge were more inclined to choose AS compared with other titles, suggesting that treatment of LRPC may increase in the future as these physicians get promoted and take control of the PCa treatment. Notably, radical radiotherapy is a preferred method to treat PCa in Europe and the United States[1], but in China, the majority of patients with PCa are primarily treated by Chinese urologists; thus, as surgeons they are biased towards surgical treatment. Our findings also support this conclusion, regarding the treatment of PCa, as 58.9% of investigators believed that surgery was most preferred to treat PCa. The survey also found significant differences among respondents from different institution types, hospitals with different annual numbers of newly admitted patients, and different familiarity with the LRPC definitions for the preferred treatments (p < 0.05). Most physicians (50.2%) in provincial or municipal level hospitals and those with 100-200 new PCa patients per year (54.9%) preferred RP. These kinds of hospitals are the second echelon in China, and these second echelon hospitals are more willing to administer RP. The largest proportions of choosing AS were observed in hospitals at the national or ministerial level (36.1%), and institutions that admitted > 200 new PCa patients per year (35.1%). These hospitals belong to China's first echelon, representing the highest medical level in the country. Their choice of LRPC treatment is basically consistent with current overseas trends, suggesting that under the influence of these first echelon institutions, the proportion of AS treatments for LRPC may change in China in the future.
Cancer has psychological effects on patients, which, in turn, affect the treatment decision. Most patients have a higher quality of life during AS than RP. However, it should not be overlooked that some patients who accepted AS have different levels of mental disorders and believed that malignant tumors exited in their body and were not being effectively treated. Under the psychological pressure of living with cancer, this fear also has a considerable negative impact on quality of life [13, 14]. One study reported that the prevalence rates of clinical anxiety and depression in patients with AS were 23% and 12.5%, respectively, compared with the prevalence rates in the local general population. Patients treated with AS had a two-fold and three-fold increase in depression and anxiety, respectively and also had more severe anxiety than patients treated in other ways[15]. One study reported that a doctors' co-decision affects patients' psychological decision-making, and patients' physical health status is inversely related to depression, neurotic personality, but positively correlated with general anxiety and PCa-specific anxiety. Higher PSA levels are significantly associated with PCa-specific depression[14]. Furthermore, a lack of partners, impaired mental health, a recent new diagnosis, influence of the clinician, and the small number of core samples collected during prostate biopsy were predictors of poor quality of life[13]. These mental states affected the patient's choice of AS. Another study found that most patients choose watchful waiting and other non-therapeutic methods, but did not choose AS[16]. The reason for preferring AS in our study was that 41.9% of patients showed cancer-related fear. Special psychological education for these patients who accepted AS might be a good way to circumvent these psychological problems, and lead to more patients actively accepting AS[13]. A total of 52.5% of patients worried about tumor progression, and 39.1% were concerned with the surgical risk, which might be reasons from both patients and doctors. We also found that 42.6% of urologists were concerned about potential medical disputes, which may be a unique reason for doctors not choosing AS in mainland China. Moreover, there was no difference in these reasons between genders, titles, or institution types, suggesting that these concerns commonly and indistinguishably exist for Chinese urologists. A further analysis discovered that personal skills, fear of surgical risk, and tumor progression were the most common factors influencing the choice of AS or RP (p < 0.05). Concern about medical disputes brought about by AS was a key factor for not choosing AS (p < 0.05). These results may be closely related to the many violent incidents against medical staff in recent years, resulting in a poor medical environment[17], and these negative events have affected the quality of life of Chinese urologists[18].
AS is more difficult to implement in China and it relies heavily on China's current guidelines. The current guidelines are the 2014 edition. Due to the large lack of Chinese clinical and basic research data, these guidelines are based on the European and American guidelines. Our research also confirmed this view; 60.8% of the respondents believed that establishing guidelines was relatively pertinent and suitable for China's actual situation, but 51.4% also considered the lack of Chinese data, and that the guidelines were based on the European and American guidelines. Even 9.2% of the physicians reported that the reference values of the Chinese guidelines are weak, and they were more willing to accept the European and American guidelines. Of course, this phenomenon will slowly change. In recent years, Chinese urologists have made rapid progress in the diagnosis and treatment of PCa[19-22], and the next edition of the guidelines will have more Chinese data. However, because of the specificity of PCa in China[23, 24], whether AS is suitable for patients with PCa on mainland China remains inconclusive[25], and whether the future guidelines will increase the proportion of AS treatments is unknown. Interestingly, the proportion of AS treatments has not risen but rather has fallen in recent years. One study reported that the proportion of patients with PCa accepting AS decreased from 4.27% in 2010-2011 to 2.33% in 2016-2017[26].
Logistic regression analysis results of whether choosing RP
| Dependent variable | Independent variable | B | S.E. | Ostwald coefficient | p | Exp(B) | Exp(B) |
|---|---|---|---|---|---|---|---|
| 95% CI | |||||||
| RP | Genders | -0.143 | 0.376 | 0.145 | 0.703 | 0.867 | 0.415-1.811 |
| Titles | 0.193 | 0.073 | 7.056 | 0.008* | 1.213 | 1.052-1.398 | |
| Hospital types | -0.003 | 0.09 | 0.001 | 0.976 | 0.997 | 0.835-1.190 | |
| ANP | -0.033 | 0.067 | 0.235 | 0.628 | 0.968 | 0.849-1.104 | |
| FLD | -0.356 | 0.097 | 13.587 | 0.000* | 0.700 | 0.580-0.846 | |
| Individual skills | 0.699 | 0.158 | 19.71 | 0.000* | 2.013 | 1.478-2.741 | |
| Surgical risk | -0.995 | 0.139 | 50.927 | 0.000* | 0.370 | 0.281-0.486 | |
| Tumor progression | 0.376 | 0.135 | 7.753 | 0.005* | 1.456 | 1.118-1.897 | |
| Medical disputes | 0.125 | 0.142 | 0.778 | 0.378 | 1.134 | 0.858-1.498 | |
| Patient loss | 0.078 | 0.2 | 0.154 | 0.695 | 1.082 | 0.731-1.600 | |
| Fear of cancer | 0.531 | 0.137 | 15.052 | 0 | 1.701 | 1.301-2.224 | |
| Other reasons | -0.651 | 0.23 | 8.029 | 0.005 | 0.522 | 0.332-0.818 | |
| Constant | 0.113 | 0.492 | 0.053 | 0.818 | 1.12 | 0.415-1.811 |
ANP=annual numbers of newly admitted patients with PCa; FLD=familiarity with LRPC definitions; RP= radical prostatectomy; CI=confidence interval
In addition, medical education of Chinese patients is generally lacking, and the outcome expectation is high[27]. In addition, the limited mobility of a large population is not conducive to regular AS follow-up. Coupled with frequent medical violence, it is difficult for Chinese urologists to withstand the potential medical disputes caused by cancer progression and metastasis during AS. Thus, it is difficult to implement AS in China.
Some limitations of this study should be discussed. The number of respondents in this study was 1,116, accounting for about 1/30 of the national urologists (about 30,000 Chinese urologists all found in the country). In addition, this study covered a wide range of China as a comprehensive survey, so the results of the study basically reflect the current actual LRPC treatment situation in China. However, the proportions of some individual provinces were too large, and the data distribution was uneven, resulting in selection bias. Furthermore, this was an online survey based on the JIU JING platform and WeChat software, which makes it unavailable for those who are not familiar with these applications.
Conclusions
LRPC is still dominated by RP in China, followed by AS. Personal skills, fear of surgical risk, and concern about tumor progression were the most common factors influencing whether AS or RP was preferred. In addition, medical disputes brought by AS are another key factor for not choosing AS. Many urologists believed that the current urological guidelines lack Chinese data. More Chinese data will be available in the future to guide treatment of LRPC.
Acknowledgements
This study was supported by the Joint Funds for the innovation of science and Technology, Fujian province (2017Y9064) and the middle-aged backbone project Health and Family Planning Commission (2016-ZQN-6). In addition, YW appreciates the great support from his wife (Weiwei WU), his son (Muyao WEI) and his mother (Shouqin XU) during the study performed and paper writing.
Author's contribution
YW prepared the draft of manuscript. XL, WS, DZ and DC reviewed the published articles. DY, SM, PZ and YW analyzed the data. LL and JJ group sponsored the study. All authors read and approved the final manuscript.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Lancee M, Tikkinen K, de Reijke TM. et al. Guideline of guidelines: primary monotherapies for localised or locally advanced prostate cancer. BJU INT. 2018
2. Cooperberg MR, Lubeck DP, Meng MV. et al. The changing face of low-risk prostate cancer: trends in clinical presentation and primary management. J CLIN ONCOL. 2004;22(11):2141-9
3. Chen RC, Rumble RB, Loblaw DA. et al. Active Surveillance for the Management of Localized Prostate Cancer (Cancer Care Ontario Guideline): American Society of Clinical Oncology Clinical Practice Guideline Endorsement. J CLIN ONCOL. 2016;34(18):2182-90
4. Iremashvili V, Pelaez L, Manoharan M. et al. Pathologic prostate cancer characteristics in patients eligible for active surveillance: a head-to-head comparison of contemporary protocols. EUR UROL. 2012;62(3):462-8
5. van den Bergh RC, Vasarainen H, van der Poel HG. et al. Short-term outcomes of the prospective multicentre 'Prostate Cancer Research International: Active Surveillance' study. BJU INT. 2010;105(7):956-62
6. Klotz L. Active surveillance for prostate cancer: for whom? J CLIN ONCOL. 2005;23(32):8165-9
7. Jiangping Wang, Qinzhang Wang. Revision and significance of the guidelines on prostate cancer in 2014. J Mod Urol. 2015(12):844-7 862.(Article in Chinese)
8. Briganti A, Fossati N, Catto J. et al. Active Surveillance for Low-risk Prostate Cancer: The European Association of Urology Position in 2018. EUR UROL. 2018
9. Klotz L. Active surveillance for low-risk prostate cancer. CURR OPIN UROL. 2017;27(3):225-30
10. Hamdy FC, Donovan JL, Lane JA. et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N Engl J Med. 2016;375(15):1415-24
11. Wilt TJ, Jones KM, Barry MJ. et al. Follow-up of Prostatectomy versus Observation for Early Prostate Cancer. N Engl J Med. 2017;377(2):132-42
12. Moschini M, Carroll PR, Eggener SE. et al. Low-risk Prostate Cancer: Identification, Management, and Outcomes. EUR UROL. 2017;72(2):238-49
13. Bellardita L, Rancati T, Alvisi MF. et al. Predictors of health-related quality of life and adjustment to prostate cancer during active surveillance. EUR UROL. 2013;64(1):30-6
14. van den Bergh RC, Essink-Bot ML, Roobol MJ. et al. Anxiety and distress during active surveillance for early prostate cancer. CANCER-AM CANCER SOC. 2009;115(17):3868-78
15. Watts S, Leydon G, Eyles C. et al. A quantitative analysis of the prevalence of clinical depression and anxiety in patients with prostate cancer undergoing active surveillance. BMJ OPEN. 2015;5(5):e6674
16. Carter G, Clover K, Britton B. et al. Wellbeing during Active Surveillance for localised prostate cancer: a systematic review of psychological morbidity and quality of life. CANCER TREAT REV. 2015;41(1):46-60
17. Zhao L, Zhang XY, Bai GY. et al. Violence against doctors in China. LANCET. 2014;384(9945):744
18. Wei YB, Yin Z, Gao YL. et al. Quality of life of Chinese urologists: a cross-sectional study using WHOQOL-BREF. HONG KONG MED J. 2015;21(3):232-6
19. Alcorn T. Yinghao Sun: leader of research on prostate cancer in China. LANCET. 2015;385(9965):321
20. Xu J, Mo Z, Ye D. et al. Genome-wide association study in Chinese men identifies two new prostate cancer risk loci at 9q31.2 and 19q13.4. NAT GENET. 2012;44(11):1231-5
21. Ren S, Peng Z, Mao JH. et al. RNA-seq analysis of prostate cancer in the Chinese population identifies recurrent gene fusions, cancer-associated long noncoding RNAs and aberrant alternative splicings. CELL RES. 2012;22(5):806-21
22. Na R, Zheng SL, Han M. et al. Germline Mutations in ATM and BRCA1/2 Distinguish Risk for Lethal and Indolent Prostate Cancer and are Associated with Early Age at Death. EUR UROL. 2017;71(5):740-7
23. Zhu Y, Yang XQ, Han CT. et al. Pathological features of localized prostate cancer in China: a contemporary analysis of radical prostatectomy specimens. PLOS ONE. 2015;10(3):e121076
24. Shangguan X, Dong B, Wang Y. et al. Management of prostate cancer patients with locally adverse pathologic features after radical prostatectomy: feasibility of active surveillance for cases with Gleason grade 3 + 4 = 7. J Cancer Res Clin Oncol. 2017;143(1):123-9
25. Xu M, Zhang L, Liang C. Is it appropriate to conduct conventional active surveillance for Asian men with low-risk prostate cancer? INT UROL NEPHROL. 2016;48(8):1287-9
26. Zhao F, Shen J, Yuan Z. et al. Trends in Treatment for Prostate Cancer in China: Preliminary Patterns of Care Study in a Single Institution. J CANCER. 2018;9(10):1797-803
27. Violence against doctors. Why China? Why now? What next? LANCET. 2014;383(9922):1013
Author contact
![]() Corresponding author: Longfei Liu, PhD, longfei_liuedu.cn, Department of Urology, Xiangya Hospital, Central South University, Changsha, Hunan 410000, PR China.
Corresponding author: Longfei Liu, PhD, longfei_liuedu.cn, Department of Urology, Xiangya Hospital, Central South University, Changsha, Hunan 410000, PR China.